
THE TRIAD OF THRIVING

This follows from The Challenges and The Hope.
First some framing. I am part of a group of amazing emergency physician in south-east Queensland who around 2018 banded together to form WRaPEM.
One of the most important pieces of work we did was to conceptualise “Synergistic Wellness”, in response to the debate on “What contributes to our wellness at work and who is responsible for it”.
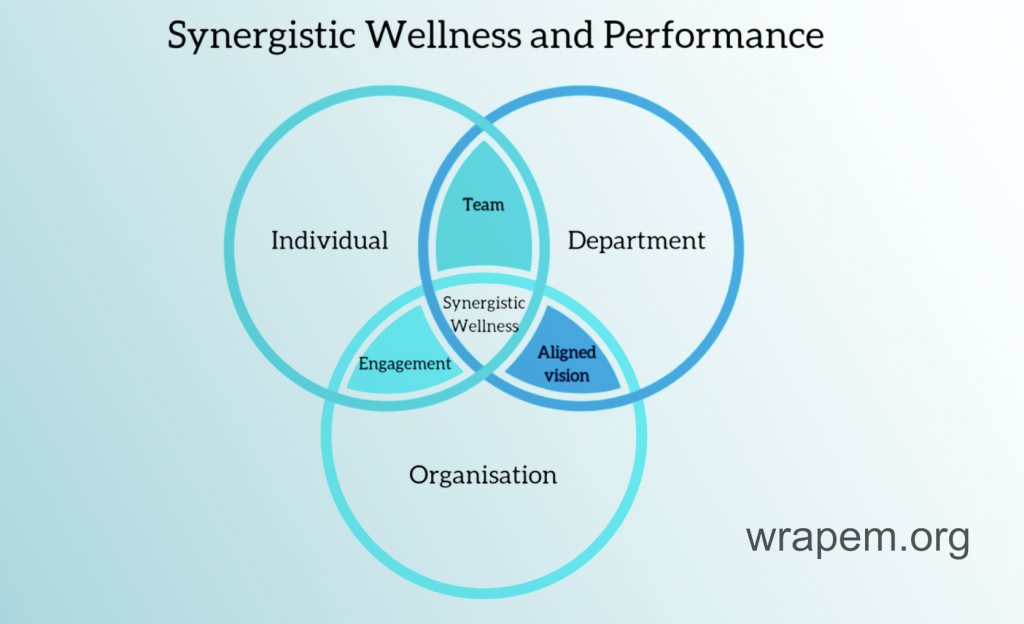
This model recognises that effective work needs to continue at organisation and departmental level, but what I’m going to focus on is this: What have I learned and practiced at an individual level that has helped me to find and maintain zest and vitality through a long career in EM?
And it comes down to a few ideas around the three pillars of meaning, connection and control, some of which may resonate with you.
Meaning
There’s a sign in a gym I used to go to that read: “When you want to quit, remember why you started.” It’s good advice for us in emergency medicine. We all started for the same reason — to do something helpful for the person in front of us. In 2025, despite the barriers, that mission remains unchanged.
As a consultant on shift, one of my methods for focusing on this mission in the midst of targets, flow and metrics is to run toward the fire – because the fire is what we are here for: a critically ill patient, a conflict, a crisis, a complaint.
I remind myself: don’t hide, no matter how much I may want to! Say “I’m coming” and go. My colleagues care about what I know and what I can do, but mostly they want me to show up.
Sometimes it’s standing elbow to elbow with our buddy as they team-lead a trauma case, or as we’re coordinating to take a toddler off their poor psychotic mother, or we conduct a hot debrief after the death of a patient.
Sometimes it’s sitting in the rubble – in the words of Liz Crowe – with a grieving family or a colleague in distress. Just sitting right there and being present. Our raw humanity is the most valuable thing that we can give, and it’s the part of our job that we can’t be paid for
Along the way, I’ve found meaning in roles outside the ED — not by design, but by opportunity. As hospital Director of Clinical Training, I underwent a steep learning curve about curriculum and accreditation, I learned to manage a team and a budget and to lobby for funding and positions. I discovered the joy and responsibility of shaping the next generation.
During the pandemic, I accidentally became the Clinical Director of a division that included ED, general medicine, public health and aged care. I managed an even bigger team with an enormous budget. Senior specialists reported to me and I learned that my value-add was of course not to give them direction but to listen, enable and coordinate.
Being an emergency physician positioned me perfectly to deal with diagnostic uncertainty in this context of a global crisis: to be decisive before we had all the information, and to balance making the correct call with making a timely call. It was exhausting – but it also revealed that meaning sometimes comes from stretching into roles that are beyond our zone comfort or imagination.
I share these undertakings hoping that you may be impressed by me. But also to recommend side-hustles like this not just to give us a break from the relentlessness of clinical emergency medicine, but also to allow us to learn and to contribute at the interface between us and ‘the broader system’.
I have of course also found huge meaning in the work around Clinician Wellness. When I look back on my career, I think – I hope – that the side hustle that comprises my most significant contribution will have been in this space (perhaps fulfilling Greenie’s prophecy!). At Gold Coast ED, we recognised that there could be no easy solution to a complex and massive problem. But we didn’t let that stop us from trying to make a start!
oneED is a departmental wellness program that was conceptualised in 2016. Nearly a decade later, its mission remains simple: to work to normalise the experience of working in emergency medicine, and to encourage people to have conversations about it. How do we do this? We do a number of things but among them: we pause at roll call once a week to do something reflective, we have flyers around our ED reminding people to take opportunities to reset in the midst of chaos and heavy load, and our name badges are branded with our logo.
Data shows that when we experience struggle, physicians tend to withdraw from others; and that, despite what we promote to our patients, we perceive stigma around feeling and discussing psychological distress. oneED tries to mitigate against the isolation that is often a part of this experience and to lessen the barriers to us asking for help.
Which brings me to Pillar number 2:
Connection
My dear friend and colleague, the late Dr Leo Marneros, used to say: It matters what you do, but what matters more is who you do it with.
I thrive because of Leo and others who continue to shape me:
Christa Bell is an emergency physician, paediatrician, and my soul sister. She is a person who is bursting with energy for life-long learning and team spirit. She reminds me that joy can be a renewable resource, whether in fun, family or the forest, and that it is contagious.
Victoria Brazil you would know to be a world-class educator and systems thinker, who taught me to zoom in and to zoom out, and who has championed me throughout my career. I have the incredible fortune to receive Vic’s almost-unconditional positive regard – although it’s also gloriously pragmatic. When I told her I aspired to one day be Governor of Queensland, she said, “I think you’d have to achieve something quite substantial to nominate for that role.”
David Green was my boss from my 2nd year as a registrar to my 19th year as a consultant. In that time, he welcomed my primly-presented self into the laid-back milieu that was Gold Coast ED in the early 2000s, he accommodated my rostering needs around a young family, and he trusted me with the freedom to experiment – and the courage to potentially fail. Can you imagine going up to your boss and saying “Hey, can we pause for a brief guided meditation at roll call on Thursday?”. Well, I did, and there was any number of things he could have said in reply, but what he said was “Er, yeah, okay. We can see how that goes”.
These relationships expanded my social capital — within the ED and across the system. I learned that being curious about colleagues, especially who they are outside of work, builds a reservoir of trust and goodwill that carries us through hard times. And that we can actively work on being the person others are glad to have on shift.
The effect of this can be so powerful. I am terrified of working in our Children’s pod — so it remains a mystery to me that everyone’s so happy to see me when I reluctantly allocate myself there! It’s a reminder that while knowledge and skill matter, simply showing up is where it starts.
A big part of that comes from fostering psychological safety: creating a vibe where juniors can say, “I’m not sure,” or even “Boss, are you sure?” and seniors can say, “I might be wrong.” So that whether we’re on our A game or flagging a little, together we’re more than the sum of our parts — and that’s how we deliver excellent care.
And finally,
Control
Experts say the antidote to burnout is engagement. I’d add a qualifier — that engagement must be highly selective.
In an overcrowded ED and across a long career with its seductive highs and despairing lows, thriving is about deliberately choosing what matters most in the moment. And being brave enough to say No to the rest.
Having optimised my spheres of control and influence, I’m now working on shrinking my sphere of concern — focusing energy where it delivers the greatest value: to patients, to our team, and to our own sustainability.
Wellness and longevity look different for each of us. One of the key ways our workplaces can enable this is to accommodate flexible career design while maintaining service provision – and I know that’s a big ask, but I’m convinced that that investment pays dividends by way of engagement, productivity and retention.
My workplace providing flexibility for me – of course balanced by some mutually-agreed trade-offs – has given me space to recharge, to nurture the elements in my life that I deeply value (family, friendships, fun), and to bring my best self back to work each time. And it also helps me feel like I can keep doing this for another 10-15 years, giving my career a long tail.
Yet we need to tread carefully. We have a fresh ACEM statement that thoughtfully guides us through workplace dialogues around evening shift and on call for later-career emergency physicians. This will be a huge advantage to me in just over three years when I turn 55. But it does shift the burden to younger emergency physicians – who may be physiologically more robust but may have young families, perhaps babies who don’t sleep, or other challenging circumstances.
And if we are not careful, they may not even make it to 55.
Supporting our junior FACEMs must be our legacy – not least because they will be the ones looking after us when we present to ED with our fractured NOFs down the track. This is the cohort that trained through a pandemic, and the ACEM surveys show that many are already cutting back or considering leaving emergency medicine. We have to pay attention to this. Thriving isn’t just us surviving — it’s ensuring others can too.
Close
So did I ever again experience elements of that first burnout episode? Of course I did.
Did I ever again write a resignation letter again? No, I didn’t.
Not because things got easier — but because I remembered why I started, who I work with, and where my real value lies: Meaning. Connection. Control.
Emergency medicine will always be chaotic. But clarity within that chaos – that’s something we can cultivate, for ourselves and for our teams, so that everyone can thrive.
I’m not the best emergency physician I know, but I’d wager that I may just about be the happiest. And that, I think, is the most honest metric of thriving in this unpredictable, messy, exhilarating and deeply human profession we all share.
Bibliography
Brindley, P. G., Olusanya, S., Wong, A., Crowe, L., & Hawryluck, L. (2019). Psychological ‘burnout’ in healthcare professionals: Updating our understanding, and not making it worse. Journal of the Intensive Care Society, 20(4), 358-362.
Elliott, R., Crowe, L., Abbenbroek, B., Grattan, S., & Hammond, N. E. (2022). Critical care health professionals’ self-reported needs for wellbeing during the COVID-19 pandemic: A thematic analysis of survey responses. Australian Critical Care, 35(1), 40-45.
2022 ACEM Sustainable Workforce Survey. Retrieved from https://acem.org.au/Content-Sources/Advancing-Emergency-Medicine/Sustaining-our-workforce/Workforce-sustainability (Nov, 2025)
ACEM’s 2025 Demographic and Workforce Profile. Retrieved from https://acem.org.au/Content-Sources/Advancing-Emergency-Medicine/Research-at-ACEM/Demographic-and-Workforce-Report (Nov, 2025)
American Medical Association. (2025). Organizational Biopsy. Retrieved from https://www.ama-assn.org/practice-management/physician-health/ama-physician-well-being-program (Nov, 2025)
Meredith, L. S., Bouskill, K., Chang, J., Larkin, J., Motala, A., & Hempel, S. (2022). Predictors of burnout among US healthcare providers: a systematic review. BMJ open, 12(8), e054243.
Rodrigues, H., Cobucci, R., Oliveira, A., Cabral, J. V., Medeiros, L., Gurgel, K., … & Gonçalves, A. K. (2018). Burnout syndrome among medical residents: A systematic review and meta-analysis. PloS one, 13(11), e0206840.
Cotobal Rodeles, S., Martín Sánchez, F. J., & Martínez-Sellés, M. (2025). Physician and medical student burnout, a narrative literature review: Challenges, strategies, and a call to action. Journal of Clinical Medicine, 14(7), 2263.
Macaron, M. M., Segun-Omosehin, O. A., Matar, R. H., Beran, A., Nakanishi, H., Than, C. A., & Abulseoud, O. A. (2023). A systematic review and meta analysis on burnout in physicians during the COVID-19 pandemic: A hidden healthcare crisis. Frontiers in psychiatry, 13, 1071397.
Hartzband, P., & Groopman, J. (2020). Physician burnout, interrupted. New England Journal of Medicine, 382(26), 2485-2487.
Shanafelt, T. D., West, C. P., Sloan, J. A., Novotny, P. J., Poland, G. A., Menaker, R., … & Dyrbye, L. N. (2009). Career fit and burnout among academic faculty. Archives of internal medicine, 169(10), 990-995.
Australasian College for Emergency Medicine Statement on Later Career FACEMs August 2025 S961 V1