
INTRODUCTION AND PRESENTING THE CHALLENGE

I wrote a resignation letter quite early in my career. It was 2002 and I was a 2nd year registrar. I addressed it to the Medical Superintendent of my hospital. In it, I stated that I was unable to continue to work where the standard of care I wanted to deliver was mis-matched with the environment available to do just that.
I never sent the letter because my ED boss, David Green, rescued me.
He explained that I was experiencing burnout, and that he’d been there too. He advised that of course I could resign if I wanted to, but that there were other options and pathways for working – and living – in a sustainable manner. His parting words to me when we met over a coffee that time were “Shahina, I think one day you’ll do something important with this”.
For the record, I realise now that I was more accurately experiencing MORAL INJURY, but I won’t condemn Greenie for not discerning that! Because it was only with my own extended learning about wellness and sustainability in medicine that I became better informed about the language and the concepts in this space.
These days, the idea of “wellness in clinical care” is not just in the collective consciousness of healthcare workers, but is articulated in workplace missions and organisational policy. While we have a long way to go, we are slowly making progress with translating these words and ideas into meaningful practice.
Many of you in this room have drafted that resignation letter — maybe not on a document,
but in your minds, at 2am on a shift that won’t end, in the space between crises. Others have figured out how to remain energetic and kick goals in every direction.
What I’d like to do is to explore how we can find ways not just to not quit, but to find and retain zest and vitality in this messy, unpredictable, intense and deeply human career.
And I’d like to do that by
– first describing our current challenges,
– then identifying where there is hope,
– and finally applying this to the learnings of my nearly-30-year journey, some of which I hope may be applicable and valuable to you.

The challenge
We have become increasingly granular in describing what strains clinicians, expanding the concept of BURNOUT into terms like moral injury, compassion fatigue and occupational stress. Yet, burnout is the term that is most widely used in the literature and so that is what I’ll call it.
The concept of burnout emerged in the late 1960s, when psychotherapist Herbert Freudenberger used it colloquially to describe the emotional stress he and his colleagues experienced caring for vulnerable patients in free clinics in the US.
It is now defined as a state of emotional, physical, and mental exhaustion produced by excessive and prolonged professional stress.
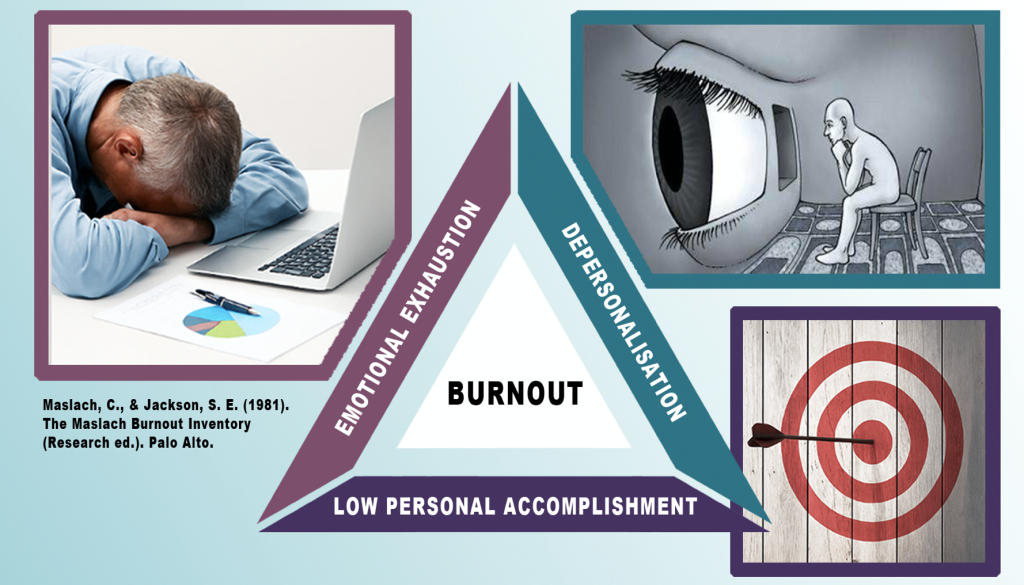
In 1981, Maslach and colleagues formulated the Maslach Burnout Inventory (MBI), incorporating three elements, all of which I could relate to with my own experience:
1. emotional exhaustion (EE) refers to feelings of overload and depletion of emotional resources; I remember recognising my physical fatigue but this emotional fatigue blind-sided me
2. depersonalization (DP) is the negative and cynical response to oneself and other people, and can contribute to detachment; at times, it felt like I stayed in my seat while my body went off and saw patients
3. reduced personal accomplishment (PA) occurs when one feels less competent in their role and less able to recognise their value and contribution; and certainly I felt like no matter how hard I worked, the waiting room remained full and the department remained chaotic, and I had not even made a dent in it
In 2015, exactly 10 years ago this issue was brought into the public spotlight when Beyond Blue published its survey on health professional wellbeing. It captured responses from about 11000 doctors and 1700 medical students and found that, when compared with the general population, we suffered psychological distress at a rate around three times higher, and suicidal ideation at a rate around double.
Since then the volume of research in this area has snowballed; healthcare professionals are said to be the most widely studied cohort for burnout (Brindley, 2019).
Data
I have mined the literature for the purpose of this piece. I found a lot of data on physicians in general, less on emergency physicians specifically, and little that compares us to other specialties. Studies are heterogeneous with respect to terminology and methodology. I also found that over the last five years, Covid has profoundly impacted the picture.
Nonetheless, the findings are globally valuable:
“What happens during a global crisis is represented within the microcosm of an ED everyday”
(Elliot at al, 2021)
The prevalence of burnout varies from study to study, but the figures reported in the 2022 ACEM Sustainable Workforce Survey are representative:
Approximately 55% of FACEMs and trainees who responded described moderate-severe burnout scores.
In next 10 years:
72% intended to decrease clinical hours of practice (62% in 2019)
and 40% intended to leave emergency medicine (27% in 2019)
This was same across age groups, except for those approaching retirement, demonstrating that even young FACEMs intended to cut back.
ACEM’s 2025 Demographic and Workforce Profile published this year (with data collected in 2024) demonstrated that this is already playing out, with only 56% FACEMs working full time.
So how do Emergency doctors compare to other specialties?
We know we can be competitive, so it may delight you to discover that If burnout were an Olympic sport, we’d win the gold medal almost every time.
In May 2025, the American Medical Association published its “organisational biopsy” ®. The report reflected data collected in 2023 from more than 18000 physicians across 43 states. Of the six specialties that reported the highest levels of burnout and job stress (emergency medicine, family medicine, obgyn, paediatric, internal medicine and hospital medicine), ED was number one.
What is it that is burning us?

A large systematic review (Meredith, 2021) explored Predictors of Burnout for all physicians. Results varied between studies, but in general it found the following:
1. Burnout was agnostic to most demographics: being a women, being married, having children, ethnicity were not linked with burnout – but younger age was possibly predictive.
2. Unsurprisingly, professional and clinical practice characteristics including workload and job stress (as assessed by longer work hours, more shifts per month, on-call time and overall higher ‘busyness’ (eg, higher patient volume per time) as well as inadequate work/life balance were associated with burnout.
And do you think salary influenced likelihood of burnout? This review found that it did not.
3. Regarding psychological health, depression and anxiety were likely to be related to burnout – but note these factors are all correlations rather than a cause or effect.
4. Physical illness/disease were likely associated with burnout. Interestingly, substance use was likely not associated with burnout EXCEPT for alcohol which was.
5. And for psychosocial variables, experiencing social stress outside of work was a factor.
For emergency doctors specifically, the 2022 ACEM data revealed this: Cramped space was sky high in our list of stressors (ED overcrowding and access block), then followed by inter-team conflict, community expectations and IT issues.
The following statement was made in an article by Rodriguez 2020 (Burnout among Residents):
“Curiously, for physicians working in urgent departments, rather than the severity of the patients, organizational factors showed a greater association with burnout syndrome”.
(Rodriguez, 2020)
Now I don’t think any of us would actually find this curious at all: on an evening shift that is adequately staffed, I can reasonably manage back-to-back critically unwell patients. What I struggle to manage is when I have to do this with 2-3 beds spaces available in a 13-bed resus pod.
Finally, is there variation according to age of the clinician?
Most studies found that burnout was higher in those aged less than 30 years. Contributing factors were listed as lack of experience and self-confidence but also economic situation, exam stress, high academic expectations, workload, lack of support. (Macaron, Meredith, Rodeles)
I postulate the additional stressor of specialist job insecurity. This year’s ACEM demographics and workforce profile showed that in 2024, a record number of FACEMs retired or withdrew ACEM membership (n=62). Meanwhile a record number of new FACEMs joined the college (n = 305). Three hundred in versus 60 out and we can see the bottlenecks we know occur for FACEM jobs especially in urban settings. I know that if were still training or early in my career, this would be a substantial source of stress for me.
By contrast, generally speaking, older clinicians report lower levels of burnout. I’m curious about why this may be although I did not find specific studies on this. Do we get better at managing ourselves, is it because we enjoy more job autonomy, or do the burnt out ones just leave? It’s likely a combination of these and other factors, perhaps the “survival of the most tolerant”…
Read on for Part 2: The Hope